
Ovarian Afunction

Ovarian afunction, along with ovarian cysts, persistent corpus luteum, and persistent follicles, is one of the acyclicities or ovarian dysfunctions. The new classification of acyclicities and ovarian dysfunctions is as follows:
- Type I Acyclicity (Ovarian Afunction)
- Type II Acyclicity (Persistent Ovarian Follicles)
- Type III Acyclicity (Follicular Cysts)
- Type IV Acyclicity (Pseudo-pregnant Corpus Luteum)
Afunction refers to a condition where the ovaries are small, flaccid, and smooth. The most critical feature is the lack of distinct functional structures, such as follicles or corpus luteum, with the absence of the latter being crucial for classification. A symptom of afunction is the absence of the estrous cycle (no estrus observed 60 days post-partum).
Afunction is a reproductive pathology that delays breeding, thereby extending the average day of lactation, resulting in economic losses on the farm. This can be checked in the RW-1 performance report from the Federation. The average number of days of lactation (denoted as dl) determines the average daily milk yield in the herd and the profitability of its production. The shorter the average day of lactation, the higher the productivity and profitability. The optimal range should be 160-180 days. A value above 200 days may indicate reproductive problems, among other things.
Causes of Ovarian Afunction
-
- Nutritional Causes:
- Energy deficiencies
- Vitamin deficiencies (vitamins A, D3, B)
- Deficiencies of micro and macro elements (sodium, calcium, phosphorus, selenium, iodine, iron, copper)
- Absorption disorders
- Metabolic Disorders Strongly Linked to Nutritional Disorders: Negative energy balance can cause metabolic disorders, primarily subclinical, such as subclinical ketosis or acidosis. These diseases can disrupt the function of many organs, including the endocrine system.
- Disorders Related to Postpartum Diseases:
Retained placenta, metritis, abomasum displacement, or clinical ketosis. - Management Conditions:
Tethered housing system, lack of movement, insufficient sunlight, or stress can also negatively impact ovarian function.
- Nutritional Causes:
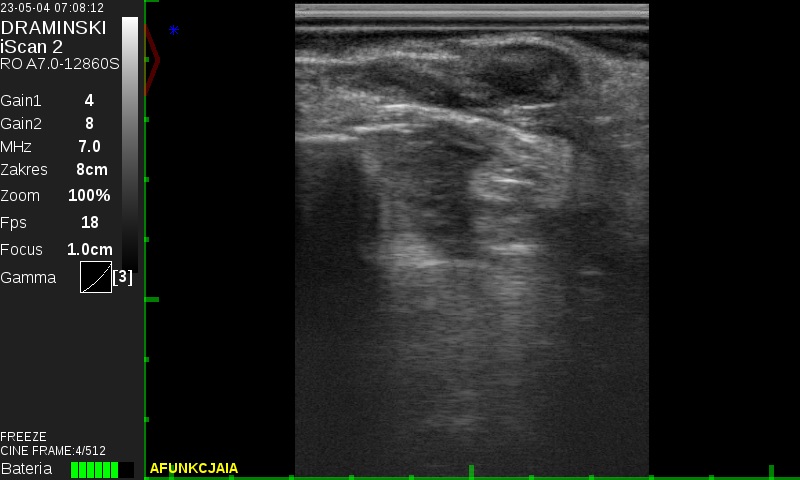
Diagnosis of Ovarian Afunction
Ovarian afunction can be diagnosed using ultrasound. On the ultrasound image, the structures appear small, with no corpus luteum and follicles measuring from a few to 9 mm or entirely absent.
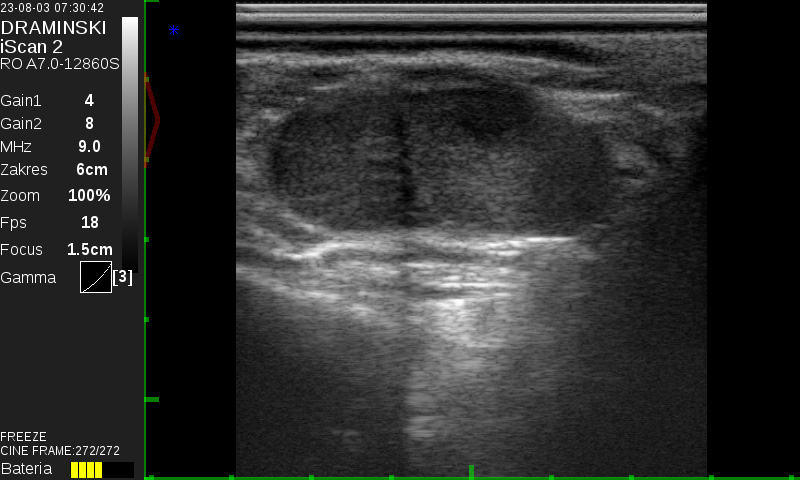
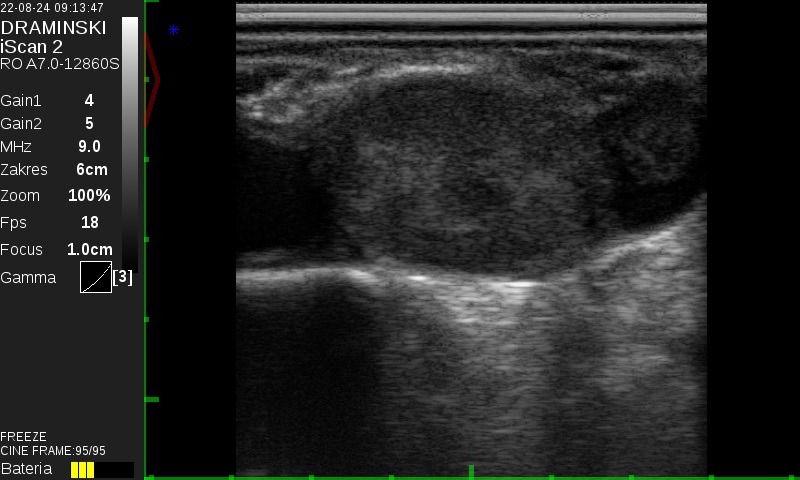
For comparison, the image of functional ovaries.
Characteristics of Afunction:
During subsequent ultrasound examinations, the size of the follicles does not change. The follicles are inhibited and do not undergo wave-like growth. The absence of corpus luteum is significant as it indicates that the estrous cycle has not occurred.
In a normal ultrasound image, ovaries without a corpus luteum and with small or absent follicles are the size of a plum.
Rectal examination alone can confirm that the ovaries are small but cannot determine whether there are structures such as follicles or corpus luteum. The confirmation test for afunction is a progesterone level test, which is low and does not increase in the case of afunction.
Treatment of Ovarian Afunction
Therapeutic options for ovarian afunction are unfortunately limited, and symptomatic treatment is often ineffective. One approach is using preparations containing hormones that act on the pituitary gland, which releases FSH and LH necessary for estrus. Other hormonal drugs directly target the ovary but are less effective for this condition. In my practice, I most commonly use a method involving gestagens combined with GnRH. As supportive therapy, I use vitamin boluses or injectable vitamin preparations.
However, it is essential to remember that no symptomatic method can be highly effective without eliminating the underlying cause.
Research Collaboration with UWM Olsztyn
I will present the results of my collaboration with UWM Olsztyn (University of Warmia and Mazury) on using ultrasound equipment to diagnose ovarian afunction, specifically to determine the size of the follicle and tailor the treatment.
I used the 4Vet mini, iScan 1, and iScan 2 devices from Dramiński to evaluate the follicles. The study was challenging as it required precise measurement of the follicle on the afunctional ovary. I examined two groups of animals:
- Those with follicles up to 9 mm (usually 3-6 mm)
- Those with follicles 9-12 mm
I used a 9 MHz probe for proper ultrasonographic evaluation of the follicles. The condition for classifying an animal for examination was always the presence of small, non-functional ovaries with an absolute lack of corpus luteum (even a small one).
Depending on the size of the follicle, I applied different treatments:
- The first group received progesterone implants for seven days, and if there was no response, the process was repeated.
- In the group with follicles above 9 mm, I used GnRH at a standard dose. Here, too, treatment was repeated if there was no response.
Conclusion:
About 10% of animals responded better to the implants, but in my opinion, time played the most significant role in both cases.
The study aimed to try to save cows that are already longer post-partum and must be treated pharmacologically; otherwise, they will be culled from the herd!
The problem of ovarian afunction cannot be solved solely through pharmacological means. It is not enough to treat only clinical cases. The entire herd must be looked at holistically—through nutrition, past diseases, and management conditions, as well as regular visits to the herd and meticulous medical-veterinary documentation. Good cooperation between the farmer and the veterinarian, and where necessary, with a nutrition advisor, is also essential.

Veterinarian: Michał Barczykowski


